Strength Training and Puberty: What Science Requires of the Physical Therapist
Reading time: 7 minutes
News

Misconception debunked by the scientific literature: resistance training in young patients does not inhibit growth. It is one of its best allies, provided it is properly supervised.
Strength training in adolescents remains a subject of persistent skepticism among the public, and sometimes among certain health professionals. Yet the evidence from the latest literature reviews is unequivocal: muscle strengthening during puberty is not only safe, it is a first-rate therapeutic and preventive tool. For the physical therapist, understanding the underlying biological mechanisms becomes an essential clinical skill.
At what age should strength training begin? Maturity before chronological age
Contemporary clinical consensus no longer sets an arbitrary minimum age. The relevant question is the child's neuro-motor and emotional maturity, not their birth date. A child able to understand and apply precise movement instructions can benefit from a structured strengthening program as early as 7 to 8 years old.
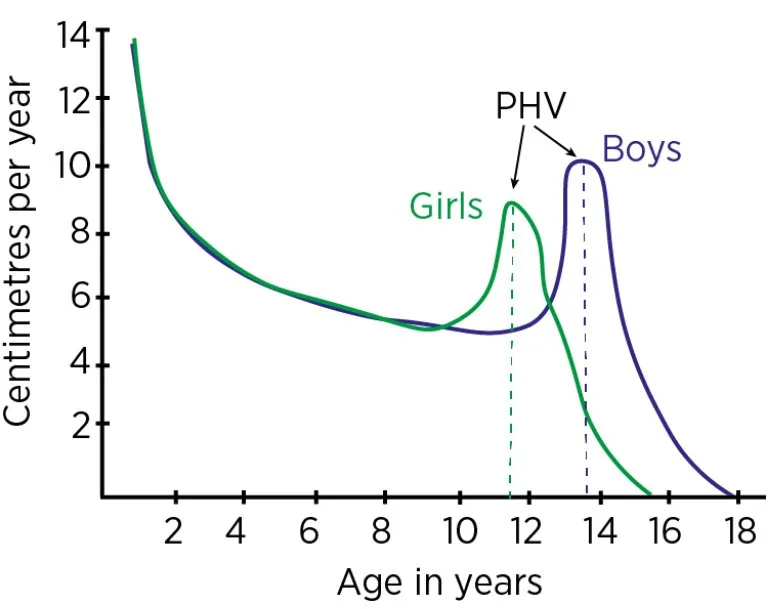
Peak Height Velocity (PHV): a unique window of opportunity
The peak height velocity (PHV), typically occurring between ages 11 and 14 in girls and 13 and 16 in boys, marks a neuro-motor window of exceptional clinical value. During this period, central nervous system plasticity is maximal, and the response to mechanical loading at the bone level is unmatched across the entire lifespan.
The challenge for the PT is not to miss this window, nor to overinvest in it without monitoring. This is precisely the role of structured, individualized follow-up.
(Source: LondonBridge Sports Medicine Group)
Bone benefits: densification, Wolff's law, and prevention of apophysitis
Contrary to persistent fears about the growth plates, controlled mechanical loading is physiologically the best available bone-stimulating intervention during growth. This principle has been known since the 19th century as Wolff's law: bone remodels according to the forces placed upon it.
Optimizing Peak Bone Mass (PBM)
It is during puberty that about 40% of an individual's total bone mineralization occurs. Mechanotransduction, the conversion of a mechanical signal into a cellular biological response, is particularly effective at this stage. Controlled studies show a significant increase in bone mineral density (BMD) in adolescents who perform resistance training, greater than that observed in trained adults under the same conditions.
Prevention of growth apophysitis
Osgood-Schlatter and Sever's disease are among the most common conditions seen in pediatric sports physical therapy. These apophysitis conditions result from excessive traction on immature bony prominences by musculo-tendinous complexes that are not yet sufficiently strengthened.
A progressive eccentric and concentric strengthening program allows better distribution of traction forces, reducing the incidence and recurrence of these conditions in a clinically significant way.
Osgood-Schlatter: progressive eccentric quadriceps strengthening
Sever's disease: calf triceps strengthening + proprioceptive training
Iliac apophysitis: lumbopelvic-femoral core stability adapted to growth
Hormonal and molecular advantages: understanding the mTOR pathway
Puberty transforms the body into a true anabolic forge. The surge in testosterone, GH, and IGF-1 creates an exceptional hormonal environment. Resistance training does not disrupt this environment: it amplifies it through specific intracellular pathways.
Factor | Role and impact during puberty |
|---|---|
Testosterone | Increased androgen receptor sensitivity, promoting post-PHV hypertrophy. The adaptive response is significant even at still modest concentrations. |
Growth Hormone (GH) | Increased post-exercise pulsatile stimulation, promoting tissue repair and linear growth. Exercise intensity directly modulates the secretory peak. |
mTOR pathway | Master switch for protein synthesis. Strength training activates mTOR through mechanotransduction, allowing gains in cross-sectional area even with still moderate androgen levels. |
The mTOR pathway: the central molecular link
The mTOR (mammalian Target of Rapamycin) pathway is the main intracellular regulator of muscle protein synthesis. This enzymatic complex responds directly to mechanical tension, converting the physical signal of resistance exercise into the production of structural proteins (actin, myosin, titin).
The major clinical value of the mTOR pathway is that it functions independently of circulating androgen levels. A prepubertal adolescent, with still very low testosterone levels, can therefore develop real functional hypertrophy through this pathway, provided the mechanical load is sufficient and properly dosed.
Direct clinical implication: monitoring training load is not optional. It is the lever that allows optimal activation of the mTOR pathway without reaching the overtraining threshold.
The role of the PT: managing load to prevent overload
For the clinician, the therapeutic goal is precise: quantify mechanical stress in order to keep the patient within their optimal adaptation zone. Growth variability during PHV, and especially the resulting strength asymmetries, requires rigorous, individualized, documented monitoring.
Strength asymmetries: an underestimated warning sign
During PHV, bone growth is faster than musculo-tendinous adaptation. This leads to often clinically silent but instrumentally measurable inter-limb functional asymmetries. These imbalances are a documented risk factor for short-term injury (strain, insertional tendinopathy) and chronic overload (apophysitis, stress fractures).
Recommended follow-up tools and strategies
Measurement of maximal isometric strength using manual or instrumented dynamometry
Assessment of agonist/antagonist ratios (especially quadriceps/hamstrings)
Quantification of training volume per session (sets × reps × load)
Monitoring of neuromuscular fatigue via RPE and countermovement jumps (CMJ)
Parental education based on objective data, essential for therapeutic adherence
Exercise prescription: structure to make it safe
Exercise prescription in adolescents must meet the same requirements as any therapeutic prescription: dose, frequency, progression, and periodic reassessment.
Digital follow-up tools now allow the physical therapist to structure this pathway rigorously, ensure continuity between in-clinic sessions and home exercise, and strengthen therapeutic education for the patient and family. Solutions such as Andrew®, dedicated to exercise prescription and patient-centered therapeutic education, make it possible to operationalize this follow-up while optimizing available clinical time.
You can also find here our article on optimizing therapeutic time through hybrid follow-up, an interesting avenue to explore with these young patients.
Practical protocols: recommendations from EBP consensus
Evidence-Based Practice (EBP) in pediatric sports physical therapy makes it possible to define clear, reproducible, and measurable recommendations. Clinicians now have a solid framework for structuring care.
Recommended training parameters by age
7–11 years: Technique first and foremost. Light loads (60–70% estimated 1RM), 2–3 sessions/week, focus on coordination and core stability.
12–14 years (pre-PHV): Progressive introduction of overload. 3 sets × 8–12 repetitions, full recovery between sets.
14–17 years (PHV and post-PHV): Structured strength training. Periodization possible, asymmetry monitoring mandatory.
Post-PHV: Adapted adult protocols, with safe access to hypertrophy and power development.
Specific precautions during the growth period
Several points of caution are specific to pediatric practice and fundamentally distinguish this population from adults:
Avoid excessive axial loading during rapid growth phases (no heavy squats, no heavy overhead press before technique is mastered)
Do not use muscle failure training in children and young adolescents
Prioritize recovery: connective tissue and cartilage adapt more slowly than the nervous system
Systematically involve parents in therapeutic education: understanding and adherence are documented clinical success factors
Medico-legal and administrative aspects: things to know
Managing a minor in sports rehabilitation imposes specific obligations, both in terms of informed consent and documentation of care
Consent and parental information
In France, physical therapy care for a minor requires parental consent. In the context of a prescription including a muscle-strengthening program, it is recommended to:
Provide parents with written information about the program's objectives, methodology, and residual risks
Document parental agreement in the patient record
Send a report to the prescribing physician at each major reassessment
Coding and billing of procedures
Rehabilitation sessions that include supervised muscle strengthening may be billed according to the NGAP based on their clinical content. When using digital follow-up and remote prescribing tools, teleconsultation opens additional billable follow-up possibilities, while also strengthening the adolescent patient's autonomy between sessions.
Conclusion: strength training during puberty, a preventive medication to prescribe
Strength training during puberty is neither a risk to manage nor a luxury reserved for elite sport. It is a first-line therapeutic and preventive tool, supported by solid evidence such as:
bone densification
activation of the mTOR pathway
prevention of apophysitis
correction of strength asymmetries.
The PT is the professional best placed to supervise this practice: musculoskeletal expertise, mastery of functional assessments, an EBP culture, and the ability to educate families. Provided care is structured with tools that match this responsibility.
A physical therapy software solution such as Andrew® makes it possible to put this approach into concrete practice: personalized exercise prescription, progression tracking, patient and parent therapeutic education, and continuity of care between clinic and home. Not to replace the clinician, but to amplify their impact.
In pediatric sports physical therapy, the best prevention of growth-related injuries is a dose of muscle strengthening, properly prescribed and properly monitored.
Article Sources